
Timothy Stange was 12 years old, growing up in Wisconsin, when his parents brought him to a doctor hoping to alleviate his Tourette’s syndrome, a neurological disorder marked by physical and vocal tics.
His neurologist, who specialized in treating children, prescribed Risperdal, an antipsychotic drug designed to treat illnesses like bipolar disorder and schizophrenia. It has never been approved by the U.S. Food and Drug Administration for treating Tourette’s.
Doctors are allowed to prescribe medications when they believe a drug may be helpful, even when the FDA has not found evidence the medication is safe or effective for that illness. In the medical world, this kind of prescription is known as being “off-label.”
For Timothy, the drug did not work as hoped.
A year after he began Risperdal, his mother took him to a pediatrician when he complained of stabbing pains in one nipple. Two years after that, Timothy had grown female-like breasts.
Classmates noticed. Timothy recounted being bullied. Six years after he first took Risperdal, the teenager needed a plastic surgeon to give him a double mastectomy, leaving him with scars on his chest.
Timothy’s plight was recounted in detail by a judge recounting the hardships he faced after taking the medication. He was far from alone.
Federal statistics show roughly 16 to 20 percent of youths suffer from mental illness and behavioral issues—including anxiety, depression, attention-deficit disorders and other conditions. Along with therapies like counseling, classroom aides and accommodations, many get medication. Often those prescriptions are off-label. Medical studies and lawsuits show adverse events are not unusual.
Off-label prescriptions are common in medicine. During the coronavirus pandemic, several have been mentioned as possible cures, though so far they have fallen short of early hopes. Donald Trump has touted supposed off-label benefits from the antimalarial medication hydroxychloroquine, which has so far proven ineffective. Treatments with the experimental Ebola drug remdesivir are also given off-label with the hope that, while unproven, they can help.
Under FDA regulations, drug companies cannot promote off-label uses directly to patients. But they can distribute studies to doctors that show an off-label use may be helpful. Several pharmaceutical companies have been accused of off-label marketing in the past decade and have even published promotional brochures and professional-journal ads.
Drugs as Mental Treatment
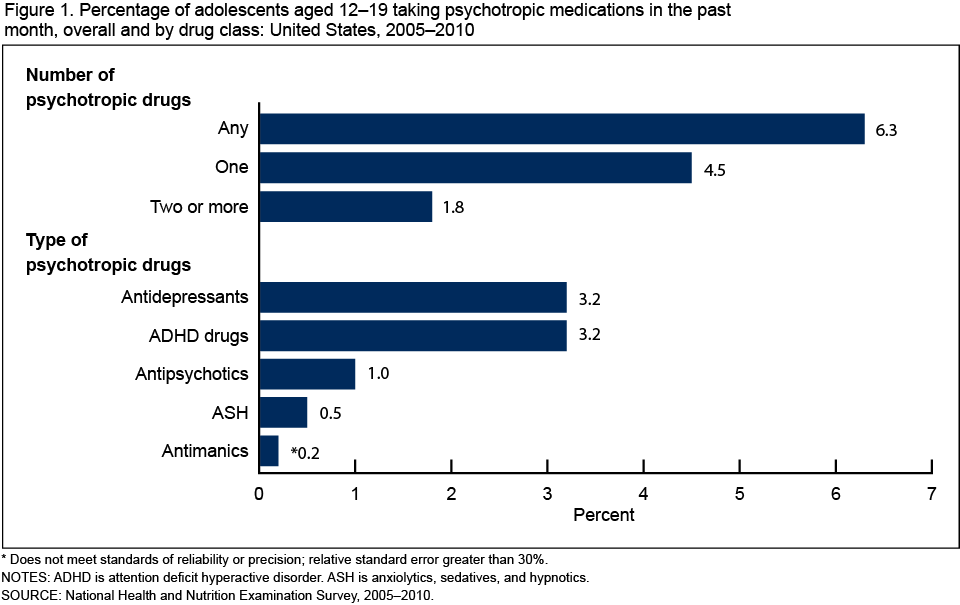
To get a sense about the widespread use of drugs to treat mental-health issues, a recent U.S. Centers for Disease Control study estimated about 6 percent of those aged 12 to 19 take drugs for treating mental illness.
The most
common pharmaceuticals for youths are antidepressants, such as Lexapro and Zoloft, and attention-disorder drugs, such as Adderall and Ritalin. A little more than 3 percent of youths are on each of these two categories of pharmaceuticals.
About one in every 100 U.S. adolescents is on an antipsychotic, making it the third most common psychiatric medication. In addition, the way antipsychotics are used also stands out: An expansive study published in 2016 estimated that two-thirds of all antipsychotic prescriptions to children and adolescents are off-label.
Other kinds of pharmaceuticals given less frequently to youths include lithium, to prevent mania; hypnotic drugs like Ambien, and anti-anxiety medications and sedatives.
To be sure, countless patients have benefited from off-label prescriptions. But the pattern of prescribing off-label antidepressants and antipsychotics to children has raised concerns in the medical profession and among patients and their families.
A study in Europe in 2019 found that while many youths benefited from antipsychotics, 12 percent experienced an adverse event. The researchers urged doctors to closely monitor side effects.
Maryland officials became so concerned about over-prescribing antipsychotic medications off-label for children that it established a review system in 2013. And concerns have encompassed not just antipsychotics but also other medications.
Parents and patients have sued drug makers for promoting off-label treatments for mental-health problems, alleging that they caused psychological damage and physical harm. Some surviving family members allege these prescriptions spurred youths to kill themselves.
Timothy Stange is among more than 13,600 who have sued the maker of Risperdal, Janssen Pharmaceuticals, a subsidiary of the drug giant Johnson & Johnson, alleging the company had hidden and downplayed evidence of bad side effects. Stange’s doctor said that while he knew Risperdal could cause a boy to grow breasts, he was under the impression this was rare.
After winning before a jury and later appeals altering the judgment, Stange settled out of court for an undisclosed sum. He declined to comment for this story, but the details of his case are in court records and a judge’s opinion.
Clinton Harper’s Journey

Clinton at age 4.
To understand how off-label prescriptions work, consider the case of Clinton Harper, who was 4 years old when he was diagnosed with autism in 1994.
“My son would not sleep,” his mother, Teresa, said in an interview. “He would stay up and he was like the Energizer rabbit. He’d never stop. He was just going and going and going and going. We had to slow him down.”
By age 6, he was on Risperdal, which at the time was not approved by the FDA for children.

With puppy, at age 6.
As part of its regulation of drugs, the FDA must approve the language put on the labels of pharmaceuticals. These labels tell doctors and patients about the benefits and risks of a drug, based on studies about effectiveness and safety.
Yet doctors are permitted to go beyond FDA-designated uses. Congress has long given doctors leeway to prescribe drugs for off-label uses.
When standard medications are not working, a doctor may believe that a drug that helps adults—even though it has not been tested on children for safety, side effects and effectiveness—could be helpful for young people.
“There are times where it is not a totally unreasonable thing to do,” said Dr. Ryan S. Sultan, a Columbia University psychiatrist who has studied the use of antipsychotic medications for children.
Off-label uses, he said, might make sense for children “getting kicked out of school regularly. They’re getting suspended. You’ve tried behavioral treatment. You’ve tried individual psychotherapy. You’ve tried parent management and you’ve tried the medications that are more likely to be helpful.”
Sultan published a study in 2019 examining prescriptions for treating attention-deficit disorder. A standard medication is a stimulant. Sultan found 2.6 percent of youths with the condition were instead on antipsychotic medications, which is an off-label use. For about half of them, stimulants—even though they are the standard medication—were never even tried.
“One of the arguments is this should never ever, ever, ever be used. And anyone who is a decent practicing clinician would say that’s ridiculous,” said Sultan. Instead, he said, it should be a “last resort.”
Clinton Harper’s doctor, Jan Mathisen, believed Risperdal would manage his symptoms. He later testified in court that he had no record of telling the boy’s mother that this use was off-label. Doctors are not required to tell patients that medications are off-label.
While Clinton was not on the verge of getting kicked out of school, the drug worked—at least for treating the manifestations of his autism, including developmental delays and behavior issues.
Then came side effects. The doctor had no record of ever warning the mother or son about bad reactions, though cautions are listed on the packaging that comes with the prescription.

By age 10, Clinton had experienced a weight gain of about 100 pounds.
In just one year, according to his mother, Clinton went from being a normal-sized kid to being “obsessed with food.” By the time he was 10, he had gained about 100 pounds. By his early teens, Teresa felt he had become too big for her to manage, and felt she needed to put him in a group home.
“My child went from a baby to a grown man in one year,” she said. “How do you prepare for that? You don’t. You can’t. You talk about some pain.”
“If I had to do it all over again, I would not have put him on Risperdal,” she said. “No, because it changed my son’s whole life.”
In 2016, doctors determined that Clinton suffered from a condition that causes enlarged male breasts.
A federal magistrate judge in 2018 sided with the drug maker in this case, writing that the law limits the liability of manufacturers, even though, Judge David A. Baker wrote, “It may well be that treatment of his underlying condition caused or contributed to a diagnosis of gynecomastia.”

Teresa Harper with her son Clinton, then 20, in 2010.
Johnson & Johnson, which now owns Risperdal, reported in securities filings in April that the company faces “significant” product liability for the drug, with about 10,900 lawsuits, though it believes it has “substantial defenses” in the court battles.
The Legal Fallout
Clinton Harper is just one of thousands of American children and teens who have gotten mental-health medications off-label.
In court, the drug companies have argued that there is little evidence their products have caused adverse events. They have denied wrongdoing when faced with allegations of ill effects from antipsychotics. The companies have sometimes blamed a patient’s diet, lifestyle or other medications.
In one of the largest healthcare fraud settlements in U.S. history, Johnson & Johnson reached a massive settlement with the Department of Justice in 2013. The company paid more than $2.2 billion to end criminal and civil allegations stemming from how it promoted Ripserdal, Invega and Natrecor. Both Risperdal and Invega are antipsychotics.
“J&J’s promotion of Risperdal for unapproved uses threatened the most vulnerable populations of our society—children, the elderly and those with developmental disabilities,” said Zane Memeger, then a federal prosecutor. “This historic settlement sends the message that drug manufacturers who place profits over patient care will face severe criminal and civil penalties.”
It was not the first case alleging improper promotion of off-label uses. In 2010, Astrazeneca paid $520 million in fines for illegally marketing its antipsychotic drug Seroquel, including to youths, according to the Justice Department.
Forest Laboratories also has faced accusations that it improperly promoted the off-label use of its antidepressants Celexa and Lexapro.
In Massachusetts, Delana Kiossovski was looking to treat her daughter’s depression when Dr. Stephen Barnett put the 12-year-old on Celexa in July 2001.
Her daughter then attempted suicide twice. Her family, in court, asserted the drug was to blame.
Kiossovski joined with another patient in 2014 to sue Forest, charging that Celexa and Lexapro were promoted for off-label use in children.
The evidence “strongly suggests that Forest engaged in a comprehensive off-label marketing scheme from 1998 through 2009 aimed at fraudulently inducing doctors to write pediatric prescriptions of Celexa and Lexapro,” US Appeals Court Judge William J. Kayatta Jr., wrote in January 2019.
This happened, he wrote, even though “Forest had insufficient reason to think that these drugs were effective for the treatment of depression in children and adolescents.”
The case was part of a massive, multi-court-district series of suits settled in February in arbitration for terms that were confidential.


{kind=link}